
|
by KIRI MACKERSEY, M.D.
All photos courtesy of Kiri Mackersey, M.D. “How about Nigeria?” The job was at a large, long-standing maternity hospital in northern Nigeria with Doctors Without Borders/Médecins Sans Frontières (MSF), an independent, medical humanitarian organization. It was my first assignment. My role would be head of the obstetric ICU and supervisor of the local nurse anesthetists in the operating rooms. MSF’s emergency obstetrics program at the Ministry of Health hospital in Jahun, Jigawa State, Nigeria, provides obstetric care and offers surgery for women with vesicovaginal fistulas. Although other areas in the north had been devastated by the ongoing conflict between Boko Haram and the Nigerian military, the security situation in Jahun was stable. The expat compound was colloquially known as Jahun Paradise and was rumored to have the best cook in MSF. I signed up. New York — Paris — Abuja — Jahun I had been warned that Abuja Airport would be a goat-filled market of chaos and danger — don’t talk to anyone after the security gate and don’t walk out with anyone, even if they say that they are a policeman. In place of livestock, however, are businessmen, tourists, families coming home and a Nigerian movie star whose entourage rivals that of the Kardashians. I spend a couple of nights in Abuja receiving security and medical briefings before heading to Jahun. The drive is about five to six hours to Jahun, depending on traffic. The drive takes seven hours on a good day … without military roadblocks. You’ll be driving for eight hours, depending on weather. Are you ready for a nine to ten hour drive, more or less? At this point, I stop asking how long the drive to Jahun will take. ICU: India Charlie We arrive in Jahun in the late afternoon. Finally I see the promised goats surrounded by a distinct lack of chaos or danger. My Australian predecessor wastes no time showing me around the hospital. I put down my bags and 10 minutes later I’m on an ICU round. The ICU has eight beds run by a local staff of two nurses and a charge nurse, Helene. At the start and conclusion of the round I am greeted with “The new med anesthetist! You are welcome.” At the door to the ICU we wash our hands and change from outside shoes into rubber clogs and white coats. The room is simple and functional, each bed separated by a nylon curtain. The head of the bed can be raised mechanically and every component can be wiped clean. There are several fans and two air conditioning units that provide welcome relief from the heat outside. We start the round immediately at bed one. Bed one: an 18-year-old G3P0 with eclampsia. She was seizing at home for about nine hours before she was brought in and delivered a deceased term baby last night. BP 185/101. No hyperreflexia, no headache. Magnesium treatment is halfway complete and she’s on labetalol. The labetalol is increased. Bed two: a 20-year-old G4P1, eclampsia. Seized again last night despite magnesium. There’s a low-grade fever and she’s drowsy and incoherent. We start a discussion: is it a postictal state, a stroke in progress, magnesium or the benzodiazepines used to break the seizure? Blood pressure is controlled, pupils equal and reactive, limbs are symmetrically hypotonic. Continue magnesium, check mag levels and electrolytes, rapid malaria screen. In my head I imagine the work-up she would receive in New York: a CT head, cultures from every orifice, anesthesia team on standby to intubate. Bed three: 25-year-old G6P3, eclampsia. She has finished magnesium treatment and is on oral antihypertensives. Northern Nigeria has one of the highest rates of preeclampsia in the world. No one knows exactly why. It could be nutritional deficiency in magnesium or a genetic predisposition, but more universal reasons, such as second marriages with multiple gestations, cannot be ruled out. The American obstetrician on our team shakes his head. He’s never seen three recently eclamptic women in the same room before. “Sahnu?” The patient in bed three nods. “Sahnu” is Hausa, the predominant language in this area. It is one of those indispensable, Swiss Army pocketknife words: how are you?/I’m fine/hello/thank you/OK/I’m sorry. By the end of my mission it forms the backbone of my vocabulary. We move on. Bed four: a 17-year-old G1P1, jaundice, abdominal distension, renal failure, lethargy, normotensive, no seizures. Her baby is in a crib beside the bed. We stand around scratching our medical heads. One of the local doctors suggests herbal toxicity. The woman has been taking a local herbal concoction of potash and plants to speed labor — her tongue is still dark from the ash. These mixtures are usually made by traditional healers and come with a high risk of liver failure. Will the lab do liver enzymes? Our new French lab technician has recently catalogued the reagents — she is hopeful. The obstetric ultrasound confirms ascites. I move up onto her chest. The curvilinear ultrasound probe just about fits between her ribs and I see a hyperdynamic, empty heart. We start IV fluids and discuss transfer to a larger state hospital. The women in beds five and six have recovered from postpartum bleeds and are ready to move to the step-down beds in the adjacent room. Helene calls their names out the window. The central courtyard is full of waiting aunts and grandmothers who feed, wash and transfer our patients. “Fatima … Family of Fatima! Come to the ICU.” A few minutes later, Family of Fatima is cloaking her in a long hijab and bright cloth “wrappa,” the traditional dress in this area. They scoop up her brightly bundled baby and walk across the doorway into the general ward. Here she will have her own bed for a couple of nights, then she will share her bed with another postpartum patient before returning to her own village. As they pass me, the women raise their hands and bow their heads: “Sahnu! Sahnu! Sahnu!” Bed seven: a 16-year-old G1P1 with anemia. Her presenting hemoglobin was 2, presenting complaint: dizziness while walking. She had delivered at home two days previously and her baby is beside her. After 4 units, the hemoglobin on our bedside fingerstick is now 6. She feels good. We debate transfusing another unit. She is nutritionally deprived and is about to spend the next few months breastfeeding. I grab the obstetric ultrasound probe (my echo). Her left ventricle is hyperdynamic and relatively empty. We take a vote and the transfusers win. We also add some high-calorie nutritional supplements. We turn to our last bed. She’s 35, G5P2 with weakness. She was brought in by her family an hour ago, unresponsive. The story is that she delivered at home overnight. She then became confused and lost consciousness in the early hours of the morning. It’s now evening. The outgoing medical anesthetist educates me: only the men drive and they may be reluctant to travel at night or in poor weather. Our admissions come in mainly between 9 a.m. and 11 a.m., regardless of the onset of symptoms. Some women travel for days, from neighboring countries, for the free, highquality care that MSF delivers. The lucky ones come by car, the rest by oxcart. Our patient flails her left side but her right side is immobile. Blood pressure is uncontrolled, Babinski’s ... I have not checked for this sign since I was a medical student. I doubt myself and repeat the test. Up-going. Her prognosis is grim. Long-term treatment facilities and rehab units do not exist in Jahun and her ongoing care will place an enormous burden on her extended family. The team is silent for a moment, deeply aware of the repercussions if no recovery is made. The static of a walkie-talkie breaks my reverie. India Charlie, this is Oscar Tango, do you copy? We copy. India Charlie, is the med anesthetist with you? We need help in Oscar Tango. Good copy, she’s coming. Operating Theatre: Oscar Tango The nurse anesthetist is struggling with an intubation. I take over and, after the tube is in, find out what is going on. Uterine rupture from a combination of eclampsia and protracted labor. Extra IV lines are secured and we cover her with a washable forced air warmer. Fresh blood is ordered from the blood bank. It arrives four minutes later, still warm from donation. In Jahun, the family of the patient “repays” by donating the number of units used by the patient. There is always a line of willing husbands and fathers on the bench outside the blood bank, waiting for a spot in the “bleeding room.” The type and screen is done on a large porcelain tablet. Blood is screened for hepatitis, HIV, syphilis and malaria. Malaria positive blood is still used — in an endemic area, too many units would be wasted otherwise — but the recipient is simultaneously treated. Packed cells are available for the neonates, everyone else gets whole blood. Hysterectomy underway, I explore the drug cabinet. It’s fully stocked with a familiar family of emergency medications. Stacks of single-use syringes and needles are neatly organized. A separate, locked shelf contains controlled substances and there is a log book in the office nearby for periodic inspections by the Ministry of Health (MOH). All controlled substance containers are discarded separately. The MOH inspector will compare the log book with the collection of vials. While I understand how narcotics and benzodiazepines made the controlled list, the reason for locking up ephedrine, caffeine and methylergometrine is more of a mystery. I turn to the anesthesia machine. I had read the orientation pack but the chrome box is quite different in practice. The nurse smiles. “Not like the one you are used to?” It reminds me of a gramophone from 1950. I follow a standard mental algorithm: first find the “on” switch. There are six dials and two pressure gauges on the Monnal D2. My predecessor points out the pressure dial, rate setting and pressure alarms. There’s an oxygen blender and an isoflurane vaporizer. Monnal has continued manufacture of these simple models as a service to medical NGOs — they are easy to maintain, easy to transport and difficult to break. In terms of the circuit, everything except the endotracheal tube is reusable. The sterilization room has a counter window into the operating theatre — central supply gives us immediate service! The next five weeks of my assignment pass quickly. I’m on call around the clock and every few days there is a soft nighttime knock at my door. Sometimes I’m called to help with mystery diagnoses (a thyroid storm, an acute non-obstetric abdomen, liver failure, psychosis mimicking a stroke) or to the operating room when a spinal won’t go in easily for an overnight C-section. I use the OB ultrasound for echo often, and rapidly discover that these young women have far from young hearts. Admissions for heart failure come in two or three times a week and some have concomitant valvular disease. I dredge up knowledge from medical school, consult my pocket pharmacopeia, and ask the local doctors if this is what a malaria spleen feels like. Every day I feel humble and grateful. How to treat burnout? Talk to colleagues, get a massage? Rest on holiday? Quit your job? Become an administrator? Perhaps. For anyone who still has the embers of medicine alight, my advice is to drop the pressures of the Joint Commission, escape the clipboards and walk away from the man who didn’t like the “feel of the pillow” in PACU. Go and treat people who ask for nothing and give only gratitude in return. I hope I helped them. There is no doubt that they helped me. ■ Kiri Mackersey, M.D., is an attending cardiothoracic anesthesiologist at Montefiore Medical Center.
0 Comments
 by MELINDA AQUINO, M.D., & SERGEY V. PISKLAKOV, M.D.
What is wellness? While many anesthesiology departments across the country have “wellness programs,” the term “wellness” has been applied in different ways. The National Wellness Institute shares the following interpretation of wellness:
explains the ability of each individual to contribute to his or her environment and community. It allows for the building of better social networks. Using this model we become able to learn the benefits of regular physical activity, healthy eating habits, strength and vitality, as well as personal responsibility, self-care and when to seek medical attention. The model encourages self-esteem, self-control, and determination as a sense of direction and helps to encourage creative and stimulating mental activities, and sharing your gifts and abilities with others.2 For years, employers have realized that on-the-job factors significantly affect workers’ ability to perform their duties appropriately and to be productive. Burnout is a known concern in terms of staff rotation and retention. Burnout is a state of emotional, mental, and physical exhaustion caused by excessive stress. It occurs when one feels unable to meet constant demands. The epidemic of burnout has spread around the world. This epidemic did not leave healthcare untouched. Significantly higher burnout rates have been found among anesthesia providers. The high incidence of burnout was reported among anesthesiology residents and academic chairpersons. Individual factors, stress, family issues and lack of a supportive community can lead to exhaustion, inefficacy, and poor clinical performance.3 Burnout can be easily mistaken for substance abuse, depression, or a personality disorder. However, in the case of burnout the symptoms are job-site related and more about dissatisfaction rather than hopelessness and withdrawal, as one finds in cases of substance abuse or depression. Those who experience burnout feel empty and devoid of motivation, and are beyond caring. Physicians experiencing burnout often don’t see any hope of positive change in their situations. If excessive stress is like drowning in responsibilities, burnout is like being all dried up. There is one additional difference between stress and burnout: while you are usually aware of being under a lot of stress, you don’t always notice burnout when it happens.4 The term “second victim” refers to the healthcare professional who experiences emotional distress following an adverse event. This distress has been shown to be similar to that of the patient — the “first victim.” It leads to burnout as well. Common reactions can be emotional, cognitive, and behavioral. The coping strategies used by second victims have an impact on their patients, colleagues, and themselves. Because of this broad impact, it is important to offer support for second victims. It is critical that support networks are in place to protect both the patient and the involved healthcare providers. “Second victims” may experience lack of respect. This may be responsible for lack of workplace motivation and employee satisfaction, increased turnover, and a lack of trust and team building among anesthesia providers. It can cause serious damage to self-esteem and the ability to contribute.5 It is the duty of the anesthesiology department’s leadership to listen, to mediate, and to be proactive in such cases. The second victims of errors often suffer in silence. Support must begin the moment an adverse event or outcome occurs. We need to facilitate the second victim’s receptiveness to receiving help and to understand the enormous emotional toll that second victims endure. Second victims have a right to participate in the process of learning from the error. The support of peers and organizational leaders is paramount. Certainly, patients and family members who are harmed come first; however, it is also important to take care of the practitioners involved in the errors, especially when they meant to do good and now find themselves in a situation where a patient has been harmed by their unintended actions. Staff needs to be aware of available resources. Second victims deserve the presumption that their intentions were good. Nobody should be blamed or shamed for human fallibility. Second victims need compassionate help to grieve and heal, and department leaders must understand the psychological emergency that occurs when a patient is unintentionally harmed. Some healthcare facilities have established special programs to prevent burnout and second victimization. These types of programs are still missing in the field of anesthesiology, however. Recently we established a Wellness Committee within the Montefiore Medical Center Department of Anesthesiology. We started by establishing a baseline for assessing staff burnout. We used the Maslach Burnout Inventory, a measurement tool that grades burnout, a three-dimensional syndrome made up of exhaustion and inefficacy.6 We also created the position of ombudsman, an individual who will advocate on behalf of the rotating students, residents, fellows and attending faculty. To ensure confidentiality and independence, the position will be held by an attending physician who is not part of the department leadership. Simple things like exercise, engaging in a hobby, and interacting with significant others are the best preventers of burnout. The role of an anesthesiology department is to enforce a respectful workplace environment. Burned out physicians can be taught the essentials of stress management and shown techniques that will enable them to deal with stress, making it manageable and thereby improving their performance and increasing their value to the department.3 The most obvious tangible benefit of supporting a colleague is an enhancement of that individual’s personal efficiency, since he or she can then focus attention on patient care and productivity. ■ Melinda Aquino, M.D., is an assistant professor of anesthesiology, pain medicine and regional anesthesiology in the Department of Anesthesiology at Montefiore Medical Center. She is co-chair of the Department of Anesthesiology’s Wellness Committee. Sergey V. Pisklakov, M.D., is an associate professor of anesthesiology in the Department of Anesthesiology at Montefiore Medical Center. He is also a member of the Department of Anesthesiology’s Wellness Committee. REFERENCES
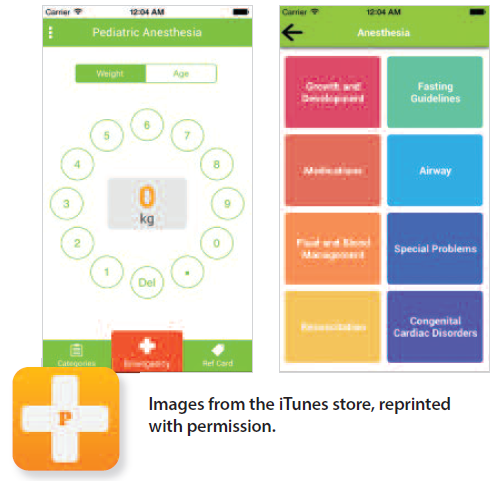 by PATRICK GARCIA, M.D. Application Name: Pedi-Anesth Cost: Free, three-day trial; $0.99 Lite $4.99 Pro Developer: Starship Review: Pedi-Anesth is a companion app developed primarily for those practicing pediatric anesthesiology. The app was developed in part by Dr. Jerrold Lerman, one of the authors of the well-renowned pediatric anesthesiology textbook A Practice of Anesthesia for Infants and Children by Charles J. Coté, Jerrold Lerman and Brian Anderson. Originally released for the Android platform, the iOS version is a port of the Android version. Like many pediatric apps, there is a thorough list of medications for weight-based dosing, organized by medication class. In addition, the app has numerous other informative sections dealing with airway equipment sizing, diagrams for congenital heart defects, difficult airway algorithms, etc. The app comes as a trialware; users have a three-day period to access the full version of the app. After the trial period, the app will prompt you to purchase either the Lite version or the Pro version. The Lite version comes with just the reference card, which provides the weight-based dose and formulas. The Pro version includes the reference card and offers the convenience of calculating the actual dose by inputting the patient’s weight. The comprehensive content in this app, with its straightforward presentation, is unmatched compared to other pediatric anesthesia apps. The sections and categories are also organized well with appropriate color schemes for better visual clarity and recognition. Other pediatric anesthesia apps are very bland in their presentation. The app has a license for use of the material from the actual textbook A Practice of Anesthesia for Infants and Children. Both the Lite and Pro versions are of great value at their price points. I did have a couple of gripes while using the app, mainly concerning the user experience. The weight selection is very unintuitive: a rotary phone layout for the numbers is confusing in this day and age — unfamiliar and unnecessary. Additionally, the transition from one section to another seemed a little more sluggish than most medical apps. The user experience is not a deal breaker, however; rather, it’s something that can easily be improved by switching to a numeric keypad from the rotary setup as well as hastening the transition speed, which I hope could be implemented in the next update. Bottom Line: Pedi-Anesth is a comprehensive app for pediatric anesthesiology providers and makes for an excellent reference. Pedi-Anesth can be downloaded from the iTunes App Store as well as the Android Google Play Store. Patrick Garcia, M.D., is a CA2 resident at SUNY Downstate. by MARK W. SAWERIS, M.D.
At a time when hospital administrators are often challenged to keep their medical systems afloat, SUNY Upstate Medical University in Syracuse, New York, is flourishing. In 2015, the hospital reported a $120 million profit (up $50 million from the previous year) on $1.02 billion in revenue, largely due to an additional 1,133 operating room cases performed. The increase in caseload requires a keen and attentive administrative effort to maintain diligence and patient safety. The Department of Anesthesiology, led by Chairman Dr. P. Sebastian Thomas, has played a significant institutional leadership role in the successful adjustment to this higher volume. Under his guidance, the department has made strides both at the institutional and state levels. As the premier institution in Central New York, there hasn’t been a more exciting time to practice anesthesia here. SUNY Upstate Medical University is a vital regional resource for an area that stretches from Pennsylvania to Albany and all the way to the northern Canadian border. The anesthesiology department serves a major leadership role in the provision of the highest level of care in the region’s only comprehensive Level I trauma center. The East Tower is the home of the newly constructed Golisano Children’s Hospital, which opened in September 2009 and has become the major referral center for a full range of pediatric services, including an acute post-operative pain service, under the leadership of Dr. Bettina Smallman. Across from the East Tower is a brand new, state-of-the-art Cancer Center, which was awarded the CEO Cancer Gold Standard accreditation. The cancer team’s mission is to promote healthy lifestyles, reduce cancer risk, and encourage early detection through advancements in cancer screening. The institution also boasts Central New York’s first and biggest comprehensive Stroke Center, with the highest designation and level of care for stroke patients with the worst possible neurological sequelae. The new facility allows for the expansion of faculty research projects, including hyperbaric oxygen treatment of brain injury, amelioration of neurologic injury after cardiopulmonary bypass, chronic pain models, and immunosuppression after organ transplantation. Additionally, these modern facilities supplement a unique residency training experience by expanding the practice of anesthesiology to new “off-site” locations. This training experience supplements many other components of the academic curriculum, including the department’s own simulation lab. The lab experience helps get trainees up to speed with common operating room emergencies, providing an instrumental transition to clinical practice. Dr. Jesus Robert Calimlim and Dr. Rahila Bilal simulate many virtual scenarios with trainees — including, for example, emergency endoscopies with uncontrolled gastrointestinal bleeding and blunt trauma requiring massive transfusion protocols — before they encounter real situations with real consequences. The program also maintains an annual dissection course in the cadaver lab with the pain fellows, a great way to master anatomical landmarks and skills needed for regional anesthesia. Dr. Bilal is one of many faculty members with IRB-approved research projects on the subject, including the study of long-term analgesia obtained from penile blocks in hypospadias repairs and circumcisions. Dr. Carlos Lopez, our program director, strongly believes in a rigorous academic curriculum. He is a passionate educator who takes all first-year categorical residents under his wing. My first encounter with Dr. Lopez occurred late in my residency interview trail. Instead of the standard one-on-one applicant and prospective program director interview (one that the majority of programs follow), he utilizes a more inclusive approach. Sitting at the edge of the table while nervous applicants made their entrance, his skill at transforming an awkward group encounter into an open group discussion (among strangers, no less) stood out to me. He is truly a gifted teacher. In his spare time, aside from residency obligations, he serves as a member of both the NYSSA’s Problem-Based Learning Discussions (PBLD) and Academic Anesthesiology committees to encourage academic discussion on important anesthesia topics. Dr. Lopez works closely with Dr. Thomas, our chairman and the vice chair of the NYSSA’s PostGraduate Assembly in Anesthesiology (PGA) Mini-Workshops Committee. Our program had 20 presentations at both the American Society of Anesthesiologists (ASA) and PGA conferences this year, thanks in part to our faculty’s heavy involvement in academic research with the residents in our program. Dr. Richard Beers, who is also a member of the NYSSA’s PBLD Committee and serves as PGA general chair, works with Dr. Lopez and Dr. Thomas to encourage academic achievements and advancements in clinical practice. As a member of the ASA’s Committee on Occupational Health, Dr. Beers helps provide guidance on the prevention of workplace illness and injuries. He recently published multidisciplinary infectious control recommendations for the operating room — in conjunction with surgeons, nurses, and pharmacists — in the May 2015 issue of the ASA MONITOR. This is a subject anesthesiologists are putting in the national spotlight while also taking a more prominent role in providing recommendations to help diminish the rampant progression of uncontrolled infectious diseases. As the fifth district delegate to the Medical Society of the State of New York and a former president of the Onondaga County Medical Society, Dr. Beers has also been active in legislative reform, specifically with regard to New York tort law and the effort to limit burdensome legal expenses in the region. SUNY Upstate Medical University has been a huge stimulus for economic growth by providing employment opportunities in its unique subspecialty service areas. These include complex spinal procedures, robotic gynecological and urological procedures, and neurological interventions, including the region’s only Gamma Knife Center. Dr. Reza Gorji, professor of anesthesiology, and Dr. Fenghua Li, assistant professor of anesthesiology and associate program director, are heavily involved in complex neuroanesthetic services and are pioneers in the advancement of intraoperative neuromonitoring. Together they published a research article in the Neurodiagnostic Journal regarding multimodality of intraoperative neurophysiological monitoring during Onyx embolization of cerebrovascular malformations. They have also worked to advance the understanding of cerebral ischemic injury in relation to repercussion injury as well as intraoperative fluid management. I personally had the privilege of working with both of them on a poster presentation regarding postoperative neuroleptic malignant syndrome secondary to pharmacological interactions in an end-stage Parkinson’s patient, to be presented at the ASA 2016 Conference in Chicago. We also have faculty and fellows from our outstanding pain management division who have written chapters in notable textbooks, including a chapter written by Dr. Vandana Sharma in Complex Regional Pain Syndrome: Past, Present and Future, published by Nova Science Publishers. Additionally, Dr. Brandon McGinn wrote a piece for the Essential Clinical Anesthesia Review regarding physiological changes in pregnancy and analgesia for labor. Drs. McGinn and Sharma, along with Dr. Parikshith Sumathi, work with residents in the block room and the Upstate Comprehensive Pain Clinic. They are instrumental in teaching the attentive skills necessary in regional and neuraxial anesthesia to provide regional blocks for operating room procedures as well as treatment for chronic low back pain syndromes, sympathetically mediated pain syndromes, CRPS, post-operative and diabetic neuralgias, deafferentation pain syndromes, phantom limb pain, cancer pain, and various myofascial pain syndromes. The pain fellowship here at SUNY Upstate is one of the largest and oldest in the state, established in 1977 and rapidly growing in size and patient load. Aside from these academic achievements and positions, our department members proudly host the NYSSA booth at the annual New York State Fair in Syracuse. For those unfamiliar with this event, it is without question upstate’s biggest attraction. Drawing nearly one million to the New York State Fairgrounds, it is conveniently located in the heart of Syracuse, the ideal location for such an event. The fairgrounds are currently undergoing a $50 million renovation to accommodate even larger crowds that are coming to watch mainstream artists like Jason Derulo and Nas, among others. In the mix of the chaos, Dr. Srinivasa Thota, the NYSSA state fair vice chair and Communications Committee member, can be found at the NYSSA booth raising awareness about the role of anesthesiologists in medical practice. In addition to his work on behalf of the NYSSA, Dr. Thota has written chapters on pituitary apoplexy for a textbook on neuroanesthesia by Elsevier publications as well as a chapter on neuroimaging and clinical monitoring for a standard reference book, Essentials of Neurointensive Care, to be published by Oxford University Press, U.K. Dr. Thota is joined at the fair by SUNY Upstate residents who volunteer their time to answer questions about the specialty of anesthesiology. This includes showing enthusiastic members of the general public airway management techniques using mannequins. Volunteer physicians inevitably offer medical advice to those who haven’t seen a doctor in years. In one instance, an intrigued elderly man, who admitted the only reason he visited the booth was to learn more about the field for his grandson, was persuaded by our chief resident to go to the emergency room for chest pain that was later diagnosed as an NSTEMI. This likely saved his life, and he was very thankful after the fact. This fairgoer and others have commented on the traction and recognition the NYSSA booth has garnered at the jam-packed event. Our department excels in advancing the mission of the New York State Society of Anesthesiologists at this annual event, while occasionally also enjoying some roasted corn, a Daniella’s lobster roll, or a Gianelli’s sausage with peppers and onions. The New York State Fair isn’t the only fun event in town. The hospital is located in close proximity to University Hill, and the faculty and staff members at Upstate Medical University are frequent visitors to the Syracuse University Carrier Dome. In the stadium that athletic icons and legends Jim Brown and Ernie Davis built, the incredible athletic program here never disappoints, including the basketball program’s improbable run from an at-large number 10 seed bid in the NCAA tournament to the Final Four. Jim Boeheim, assistant coach of the USA Olympic men’s basketball team and legendary coach of Syracuse basketball, is nearing retirement. He is a frequent visitor to the Golisano Children’s Hospital here at SUNY Upstate, to the excitement of patients and staff alike. A great role model and incredible icon, he embodies everything people love about Syracuse. He is a big supporter of and an advocate for the institution. Under his guidance, the hospital and private university often throw joint fundraisers for children with incurable malignancies. In addition to serving the NYSSA at a regional level, members of the institution are invigorating their approach to treating uncontrolled diabetes, a national epidemic that affects 29 million people. SUNY Upstate has officially reinstated its pancreatic transplant program under the leadership of Dr. Rainer Gruessner, chief of the Transplant Surgery Program, and the results are promising. As an advocate of pancreatic transplant in the definitive treatment of diabetes, it was Dr. Gruessner’s goal to reinstitute this program after a prolonged dormant period. To that end, the institution recently (and successfully) performed its first pancreatic transplant since 2005. The reinstitution of pancreatic transplant surgery reaffirms SUNY Upstate’s reputation as the leader in the region for combating endocrine disease. The procedure offers a cost-effective alternative to the rampant medical costs accumulated secondary to diabetic end organ damage. This cost-effective approach has been made possible through advancements in population health management tools and partnerships with healthcare providers to share analytics on clinical interventions aimed at key patient groups, including those with diabetes. Upstate University Hospital was recently listed as a 2016 “Most Wired” hospital by Hospitals & Health Networks (H&HN), a publication of the American Hospital Association. This has been a great breakthrough for our anesthesiology department, as advancements in IT continue to improve the infrastructure and quality performance necessary for the residency training program to achieve both value-based and educational healthcare. For example, it is through IT advancements that the institution can promote the immunosuppressive protocols in the operating room that are necessary for successful procedures. The transplant program not only adds to our training, it also offers a promising alternative to combat one of our nation’s biggest health epidemics. It’s an exciting time to be a resident here at SUNY Upstate Medical University and a member of the Syracuse community. The cliché, “If you can make it here, you can make it anywhere” certainly applies for SUNY Upstate, an institution that is experiencing incredible growth and achievement. I am thankful for my time here and will continue to enjoy watching this program grow to new heights. Mark W. Saweris, M.D., is a CA2 resident at SUNY Upstate Medical University from the Long Island and New York City region who loves all that Central New York has to offer. Photographs courtesy of SUNY Upstate Medical University. |
Photo from markus spiske
